
Urinary tract infection (UTI) is defined as the presence of >10^5 microorganisms/ml of urine in the urinary tract in a midstream sample of urine. UTIs are quite common worldwide, but more prevalent in the developing
and underdeveloped countries. Both makes and females are suffer from
urinary tract infections, but females are generally more susceptible to
UTIs. Causes of increased occurrence of UTIs in females : Other risk factors that may affect both sexes : Some common organisms causing urinary tract infections : Clinical Features of UTIs : It is important to remember that some patients show no symptoms despite having an UTI. This is known as asymptomatic bacteriuria. Depending on the location of infection along the urinary tract, UTIs can be divided into Upper UTI and Lower UTI. Upper UTI commonly presents with fever with chills and rigors and,
loin pain and tenderness. Lower UTIs commonly presents as fever, burning
sensation during micturition and suprapubic pain. Long standing upper UTI may cause renal damage. No such risk with lower UTIs. For upper UTIs, usually parenteral antibiotics for long duration is
necessary. For lower UTIs, usually oral antibiotic for short duration is
enough. Some typical features of lower urinary tract symptoms : Laboratory Investigations : Treatment : In general, trimethoprim is the 1st choice drug for uncomplicated UTIs. Other drugs include amoxicillin, cephalexin, ciprofloxacin, etc. For complicated UTIs, co-amoxiclav and ciprofloxacin are the first choice drugs. cefuroxime and gentamicin are also used. Important thing to keep in mind is that, trimethoprim and quinolones like ciprofloxacin should be avoided in pregnant ladies. Drug of choice in pregnant ladies are cephalexin, amoxicillin and co-amoxiclav. Recurrent Urinary Tract Infections : If the causative organism persists on repeat culture despite
treatment, or if there is reinfection with any organism after an
interval, then an underlying cause is more likely to be present and a
more detailed investigation may be necessary. In women, recurrent UTIs are common. So, further
investigation is only justified if the frequency of infections are 3 or
more per year or if theinfections are unusually severe. Recurrent UTI,
particularly in presence of an underlying cause may result in permanent
renal damage. Prophylactic therapy : If an underlying cause can not be removed, suppressive antibiotic
therapy can be used to prevent recurrence and reduce the risk of
septicemia and renal damage. Urine should be cultured at regular
intervals. A regime of 2 or 3 antibiotics in sequence, rotating every 6
months is used in an attempt to try and reduce the risk of emergence of
resistant organisms. Trimethoprim, co-amoxiclav and nitrofurantoin are some commonly used drugs. Prophylaxis against recurrent UTIs : Essentially, we should all try to adopt these habits, regardless of whether one suffers from recurrent UTIs or not. Sources :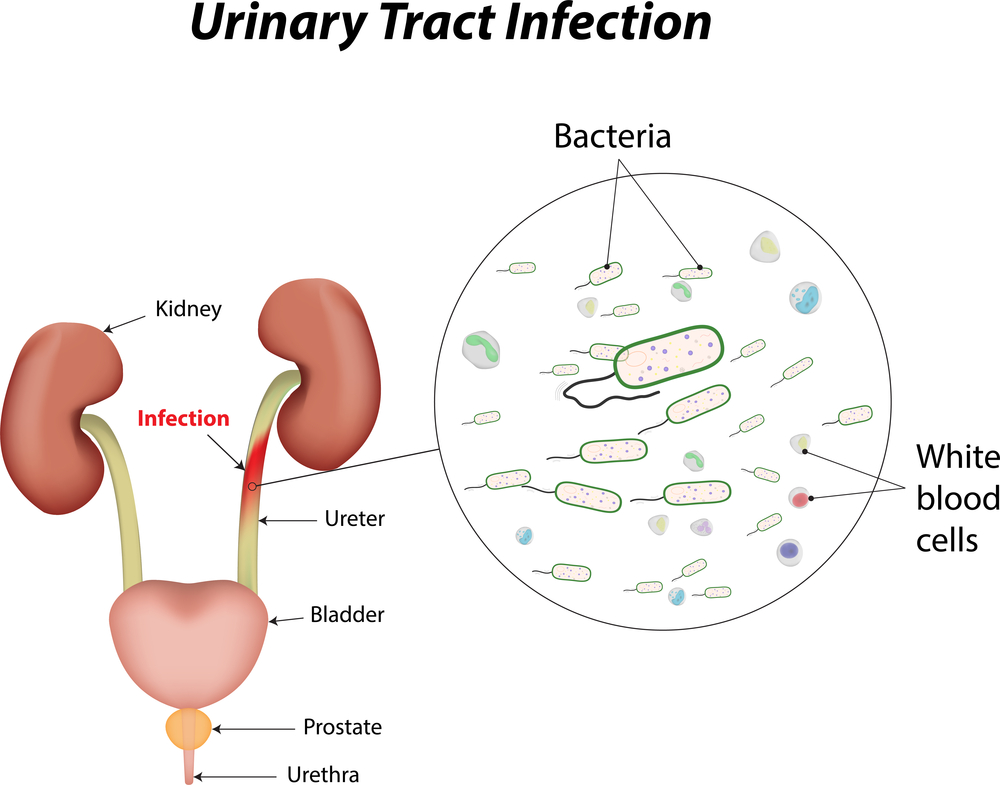
image from bing
a) Bladder outflow obstruction
b) Neurological problems like multiple sclerosis, diabetic neuropathy.
c) Vesico-ureteric reflux
a) Atrophic urethritis and vaginitis in post menopausal women
b) Diabetes Mellitus
a) Staph. Saprophyticus causes UTIs in newly sexually active females.
B) Staph. Epidermidis is responsible for UTIs associated with indwelling urinary catheters.
Infections of the kidney and ureters are classified as Upper and anything below the ureters are Lower UTI.
a) Hesitancy (worsened if the bladder is very full)
b) Poor flow, which is unimproved by straining
c) Intermittent stream : stops and starts
d) Dribbling, including even after micturition
e) Sensation of poor bladder emptying
a) Frequency
b) Nocturia : Excessive frequent urination after going to bed
c) Urgency
d) Urge incontinence
e) Nocturnal incontinence (enuresis) : Involuntary discharge of urine
after the age at which bladder control should have been established
A full course of appropriate antibiotics should be prescribed to treat
UTIs. Specific treatment regimens varies widely depending on the
specific organism that is causing the infection and their sensitivity
and resistance to the available antibiotics.
Davidson's Principles and Practice of Medicine, 22nd edition
D.C. Dutta's textbook of Gynecology, 6th edition
Bailey and Love's Short Practice of Surgery, 26th edition
Goljan Rapid Review Pathology, 4th edition
Taber's Cyclopedic Medical Dictionary, edition 21
0